|
Airway Management in a Critical Care Transport System: A Retrospective Analysis of First Attempt Success and Adverse Events
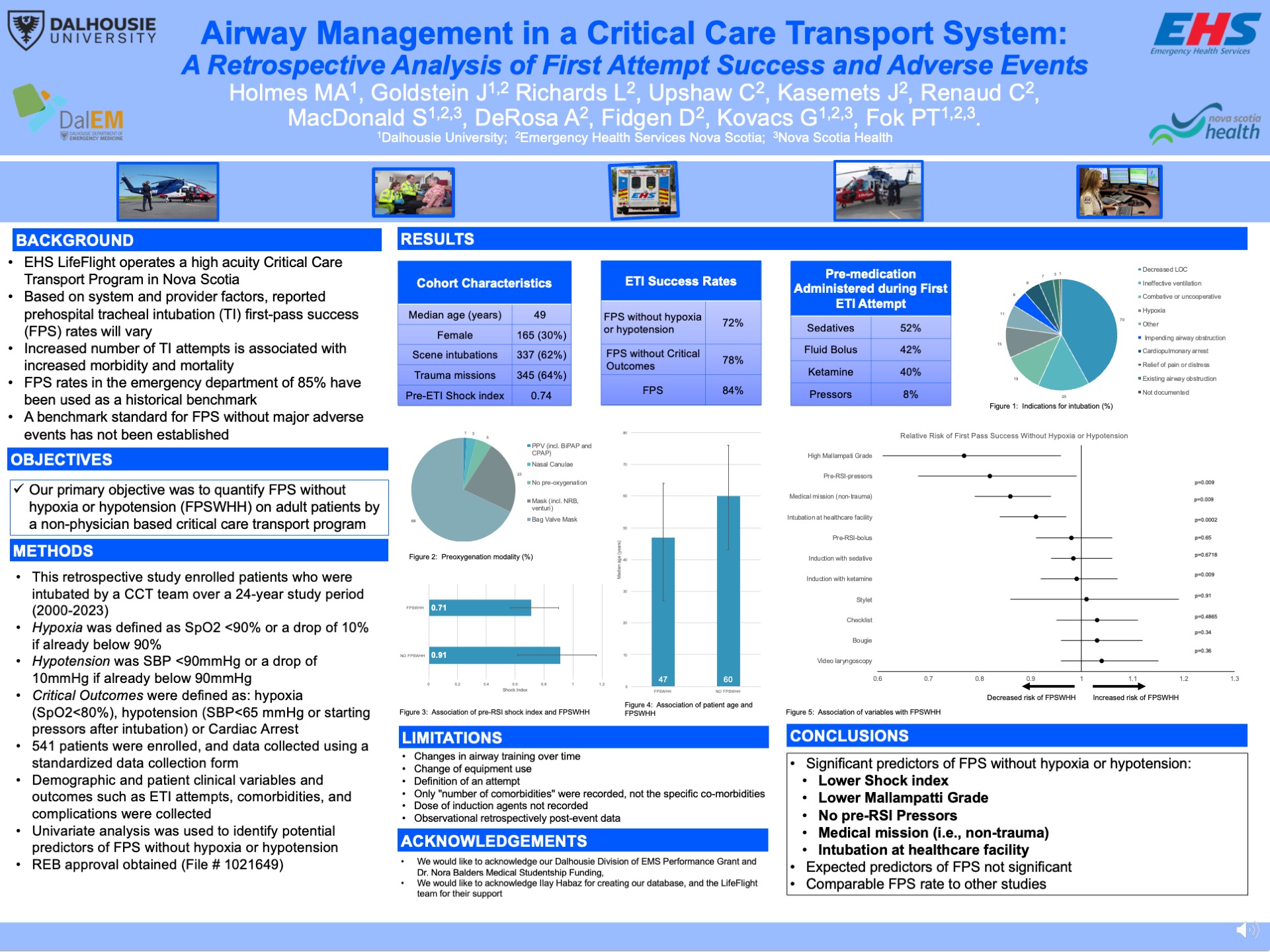
Introduction: Canadian Critical Care Transport (CCT) teams routinely perform endotracheal intubation (ETI) as part of their airway management strategies. First pass success (FPS) is the reporting standard, as multiple ETI attempts are associated with worse patient outcomes. Rates of FPS in out-of-hospital ETI vary based on system and provider characteristics, with a benchmark of 85% based on Emergency Department data. Hypoxia and hypotension have also been associated with increased mortality and morbidity. To reflect the importance of avoiding these complications, the outcome of Definitive Airway ‘sans’ hypoxia/hypotension- on first attempt (DASH-1A) has been described, but not established, as a new standard.
Objectives: Our primary objective was to quantify DASH-1A, defined as FPS without hypoxia (SpO2<90% or drop of 10% if below 90 mmHg) or hypotension (SBP <90 mmHg or drop of 10% if already below 90 mmHg), in our high-acuity CCT program.
Methods: We conducted a health records review of patients who were intubated by our CCT team over a 24-year period. Descriptive statistics were used to analyze the patient population, intubation, and complications variables. The primary outcome was DASH-1A; secondary outcomes were FPS and FPS without critical outcomes (SpO2<80% or SBP<65 mmHg). The secondary objective was to identify patient and mission variables that were associated with DASH-1A.
Results: A total of 541 patients were enrolled. Overall FPS rate was 84% [81-88]. DASH-1A was 72.3%; [68.5-76.1]. ETI-related hypotension, hypoxia, or both occurred in 9.1% [6.7-11.5], 3.9% [2.3-5.5], and 1.5% [0.5-2.5] of patients. Univariate analysis identified age, shock index, Mallampati score, pre-ETI vasopressors, medical missions, and intubation at a healthcare facility were associated with a decreased risk of DASH-1A.
Conclusion: Our results support the safety of ETI in a high-acuity CCT Program. Our CCT teams have a high rate of FPS with few adverse events, though DASH-1A rates were lower than simply measuring FPS. Multiple patient and mission characteristics were associated with DASH-1A. We propose that future CCT performance reports should include standardized reporting of clinically significant outcome measures, such as DASH-1A, allowing for between system differences.
|